
The Complete Guide to Tinnitus Relief: Everything You Need to Know
A comprehensive, science-based guide to understanding and managing tinnitus. Learn what works, what doesn't, and how to reclaim your life from the ringing.
By Yuan Liu, MD
Table of Contents
Part I: Understanding Your Tinnitus
- Chapter 1: What Is Tinnitus, Really?
- Chapter 2: The Neuroscience of Phantom Sounds
- Chapter 3: Types and Classifications
- Chapter 4: Common Triggers and Causes
Part II: The Medical Landscape
- Chapter 5: When to See a Doctor
- Chapter 6: Diagnostic Tests and What They Mean
- Chapter 7: Medical Treatments: What Works, What Doesn't
- Chapter 8: The Truth About "Cures"
Part III: Evidence-Based Management
- Chapter 9: Cognitive Behavioral Therapy: The Gold Standard
- Chapter 10: Sound Therapy and Masking
- Chapter 11: Mindfulness and Meditation
- Chapter 12: Sleep Strategies That Actually Work
Part IV: Living Well With Tinnitus
- Chapter 13: Diet, Exercise, and Lifestyle Factors
- Chapter 14: Protecting Your Hearing
- Chapter 15: Technology and Apps
- Chapter 16: Building Your Support Network
Part V: The Future
- Chapter 17: Emerging Treatments
- Chapter 18: Your Personal Action Plan
Introduction: A Letter to Someone Who Can't Sleep
It's 3:17 AM, and you're reading this because the ringing won't stop.
I know because I've sat across from many patients who've described this exact moment. The desperation. The exhaustion. The feeling that you're going crazy while the rest of the world sleeps peacefully.
You've probably already tried the supplements. Searched "tinnitus cure" at ungodly hours. Maybe you've even considered those expensive devices advertised on late-night TV. You're not alone. Tinnitus affects millions of Americans, and I've spent my career as a neurotologist trying to help people navigate it.
This guide represents everything I've learned from peer-reviewed research, clinical practice, and patients who've successfully reclaimed their lives from tinnitus. Not everyone's tinnitus can be cured, but many people can reduce the suffering it causes. That is the practical hope the evidence supports.
Part I: Understanding Your Tinnitus
Chapter 1: What Is Tinnitus, Really?
Let's start with what tinnitus isn't. It's not a disease. It's not a sign you're going deaf (usually). And despite what that relative told you at Thanksgiving, it's definitely not "all in your head."
Tinnitus is a symptom—a perception of sound without an external source. Think of it as your auditory system's equivalent of phantom limb pain. Just as amputees might feel sensations in a missing limb, your brain can "hear" sounds that aren't there.
The Symphony of Symptoms
Patients describe their tinnitus in remarkably diverse ways:
- Ringing (the description people mention most often)
- Buzzing (like electrical interference)
- Whooshing (often pulsatile, matching heartbeat)
- Clicking (usually muscular in origin)
- Hissing (like steam or static)
- Roaring (low-frequency, like distant traffic)
- Musical hallucinations (rare but real—entire melodies)
The sound might be constant or intermittent, in one ear or both, high-pitched or low. This variety isn't random—it tells us something about what's happening in your auditory system.
The Volume Problem
Here's something that surprises patients: when we actually measure tinnitus loudness using psychoacoustic matching, it's often only modestly above the hearing threshold. Yet it can feel overwhelming.
Why? Because unlike external sounds, tinnitus has no "off" switch. Your brain can't tune it out like it does with your refrigerator's hum or traffic noise. It's processed differently, engaging emotional and attention centers that external sounds don't typically activate.
Chapter 2: The Neuroscience of Phantom Sounds
To understand tinnitus, we need to journey into your brain. Don't worry—I'll be your guide, and I promise to make this fascinating rather than frightening.
The Auditory Highway
Sound normally travels like this:
- Sound waves enter your ear canal
- Eardrum vibrates
- Middle ear bones amplify the vibration
- Cochlea (inner ear) converts vibrations to electrical signals
- Auditory nerve carries signals to the brain
- Auditory cortex interprets the signals as sound
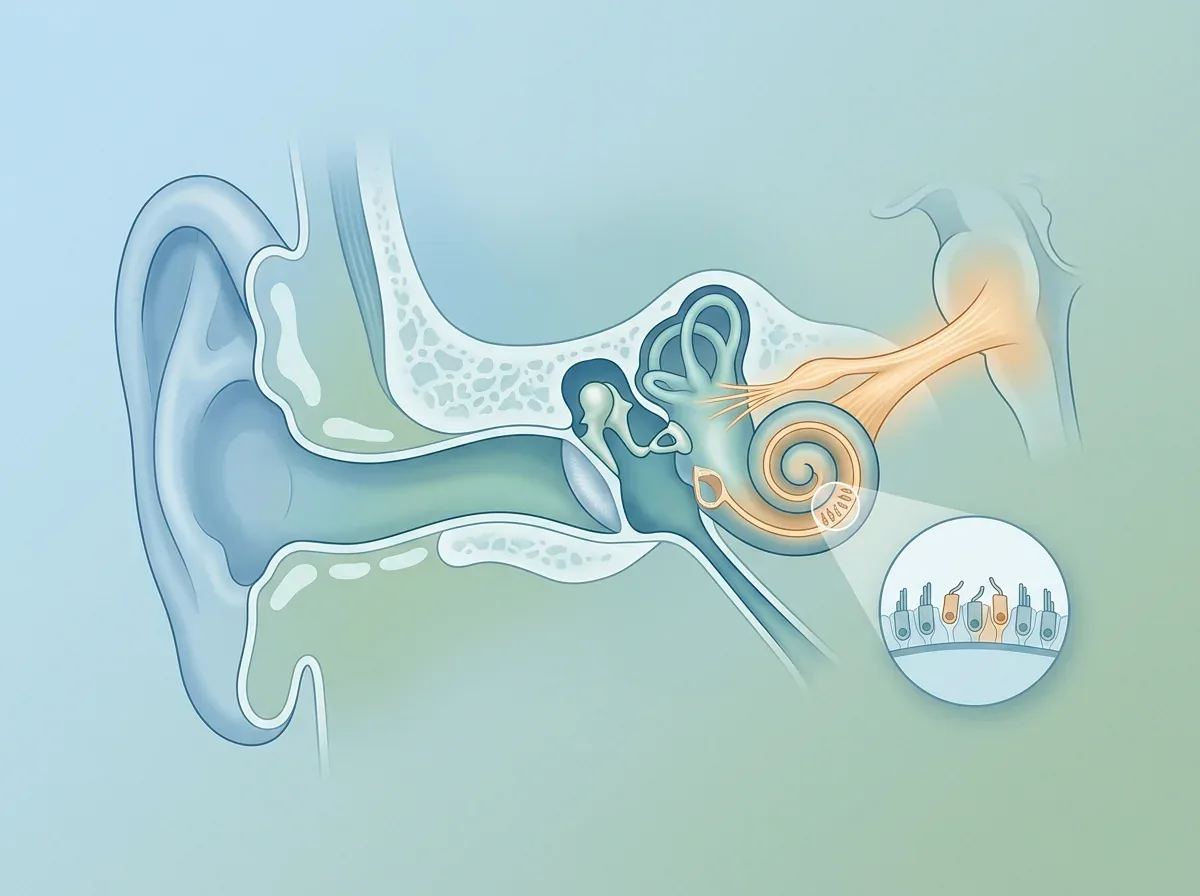
With tinnitus, this highway has a glitch. Sometimes it's damage to the cochlea's hair cells. Sometimes it's hyperactivity in the auditory nerve. Often, it's the brain itself generating signals in the absence of input—like a radio trying to find a station in static.
The Brain's Role: It's Complicated
Recent neuroscience research has revolutionized our understanding. Tinnitus isn't just an ear problem—it's a brain network problem involving:
The Auditory Cortex: Where sound is processed
- In tinnitus, shows increased spontaneous activity
- "Fills in" missing frequencies with phantom sounds
The Limbic System: Your emotional center
- Assigns importance to the tinnitus
- Triggers anxiety and distress responses
The Autonomic Nervous System: Fight-or-flight response
- Elevates stress hormones
- Increases tinnitus perception during stress
The Default Mode Network: Your brain at rest
- Hyperactive in tinnitus patients
- Associated with rumination and distress
This is why tinnitus isn't just about sound—it's about how your entire brain processes and responds to that sound.

Neuroplasticity: Your Brain's Superpower
Here's the good news: your brain is remarkably adaptable. The same neuroplasticity that allows tinnitus distress circuits to strengthen also makes it possible to retrain your response to the sound.
Neuroimaging and behavioral studies suggest successful tinnitus management is associated with:
- Less emotional reactivity to the sound
- Better top-down attention control
- Less constant checking and rumination
Chapter 3: Types and Classifications
Not all tinnitus is created equal. Understanding your specific type helps determine the best treatment approach.
Subjective vs. Objective
Subjective Tinnitus (the vast majority of cases)
- Only you can hear it
- Usually neurological in origin
- What this guide primarily addresses
Objective Tinnitus (rare)
- Your doctor can hear it too (with a stethoscope)
- Has a physical source (blood vessel, muscle spasm)
- Often treatable by addressing the cause
Primary vs. Secondary
Primary Tinnitus
- Idiopathic (no identifiable cause)
- Often associated with hearing loss
- Sensorineural in nature
Secondary Tinnitus
- Clear underlying cause
- Examples: ear infection, TMJ, medication side effect
- May resolve when cause is treated
Acute vs. Chronic
Acute Tinnitus (less than 6 months)
- Higher chance of spontaneous resolution
- More responsive to early intervention
- Critical window for treatment
Chronic Tinnitus (more than 6 months)
- Requires long-term management strategies
- Focus shifts from cure to control
- CBT becomes particularly important
Chapter 4: Common Triggers and Causes
Understanding what triggers your tinnitus is like having a weather forecast for your ears—it helps you prepare and adapt.
The Big Four Causes
1. Noise Exposure (The Leading Culprit)
- Single acoustic trauma (explosion, concert)
- Chronic exposure (occupational, recreational)
- Hidden hearing loss (normal audiogram, damaged synapses)
Prevention is everything here. Once those hair cells are damaged, they don't regenerate (yet—see Chapter 17 on emerging treatments).
2. Age-Related Hearing Loss
- Affects 1 in 3 people over 65
- Gradual high-frequency loss
- Brain "fills in" missing frequencies with tinnitus
3. Earwax and Obstructions
- Simple but overlooked
- Easily treatable
- Always check this first
4. Medications (Over 200 Can Cause Tinnitus)
- Aspirin (high doses)
- Certain antibiotics (gentamicin, vancomycin)
- Loop diuretics
- Some antidepressants
- Chemotherapy drugs
Common Triggers That Worsen Existing Tinnitus
I ask patients to track these for two weeks—patterns often emerge:
Stress and Anxiety
- Creates a vicious cycle
- Elevates stress hormones
- Increases neural hyperactivity
Sleep Deprivation
- Lowers tolerance threshold
- Impairs cognitive coping
- Disrupts neural recovery
Caffeine and Alcohol
- Individual variation huge
- Some improve with reduction
- Others see no change
Salt and Blood Pressure
- High sodium increases fluid retention
- Can affect inner ear pressure
- Particularly relevant for Ménière's disease
TMJ and Jaw Clenching
- Proximity to ear structures
- Shared nerve pathways
- Often worse in morning
Silent Reflux
- Stomach acid reaches throat/ears
- Often undiagnosed
- Night symptoms common
Part II: The Medical Landscape
Chapter 5: When to See a Doctor
Let me be direct: some tinnitus requires immediate medical attention. Here's your decision tree.
See a Doctor Within 24 Hours If:
- Sudden onset tinnitus in one ear with hearing loss
- Tinnitus after head trauma
- Tinnitus with dizziness, facial weakness, or severe headache
- Pulsatile tinnitus (whooshing with heartbeat)
See a Doctor Within a Week If:
- New onset tinnitus lasting more than a few days
- Tinnitus affecting only one ear
- Tinnitus with ear pain or drainage
- Rapidly worsening tinnitus
Schedule a Routine Appointment If:
- Chronic tinnitus affecting quality of life
- Questions about treatment options
- Need for hearing evaluation
What to Expect at Your Appointment
Come prepared. Doctors have limited time, and tinnitus consultations are complex. Bring:
- Timeline of onset and progression
- List of medications (all of them)
- Description of your tinnitus (pitch, pattern, triggers)
- Impact on daily life (sleep, work, mood)
- Previous treatments tried
Your doctor should perform:
- Otoscopic examination (looking in your ears)
- Basic hearing test
- Neurological screening
- Blood pressure check
- Neck/jaw examination
Chapter 6: Diagnostic Tests and What They Mean
The testing labyrinth can be confusing. Here's what each test tells us (and what it doesn't).
Audiometry (Standard Hearing Test)
What it measures: Hearing thresholds at different frequencies What it reveals: Hearing loss patterns, asymmetries Limitation: Can be normal despite tinnitus
Tympanometry
What it measures: Middle ear function What it reveals: Fluid, eustachian tube dysfunction Limitation: Normal in most tinnitus
Otoacoustic Emissions (OAE)
What it measures: Inner ear hair cell function What it reveals: Cochlear damage even with normal hearing Why it matters: Can detect "hidden hearing loss"
Auditory Brainstem Response (ABR)
What it measures: Nerve pathway integrity What it reveals: Retrocochlear problems, acoustic neuroma When ordered: Asymmetric tinnitus or hearing loss
Imaging Studies
MRI with Contrast
- Gold standard for ruling out acoustic neuroma
- Shows soft tissue detail
- When ordered: Unilateral tinnitus, asymmetric hearing loss
CT Scan
- Better for bone abnormalities
- Radiation exposure consideration
- When ordered: Suspected otosclerosis, temporal bone issues
CT Angiography/MR Angiography
- Visualizes blood vessels
- When ordered: Pulsatile tinnitus
Blood Tests: Sometimes Useful
While no blood test diagnoses tinnitus, these can identify contributing factors:
- Thyroid function (hypo/hyperthyroidism)
- Vitamin B12 (deficiency causes neurological symptoms)
- Complete blood count (anemia can cause pulsatile tinnitus)
- Autoimmune markers (autoimmune inner ear disease)
Chapter 7: Medical Treatments: What Works, What Doesn't
Time for brutal honesty about medical treatments. I'll tell you what I tell my patients: the evidence is mixed, and nothing works for everyone.
Medications: The Disappointing Truth
No FDA-Approved Drugs for Tinnitus Despite what you might read online, there's currently no pill specifically approved for tinnitus. Here's what we know about commonly prescribed medications:
Antidepressants
- Evidence: Mixed, mostly negative for tinnitus volume
- May help: Associated depression/anxiety
- Common types: SSRIs (sertraline), tricyclics (nortriptyline)
- My take: Only if depression coexists
Benzodiazepines
- Evidence: Can reduce tinnitus temporarily
- Major concern: Addiction potential, tolerance
- Common types: Alprazolam, clonazepam
- My take: Short-term only, if ever
Gabapentin
- Evidence: Weak, may help specific subtypes
- Best for: Acoustic trauma-induced tinnitus
- Side effects: Drowsiness, dizziness
- My take: Worth trying in select cases
Steroids
- Evidence: Strong for sudden hearing loss with tinnitus
- Window: First 2 weeks crucial, diminishing returns after
- Delivery: Oral or intratympanic injection
- My take: Absolutely for sudden onset
Supplements: Separating Hope from Hype
Americans spend millions on tinnitus supplements. Here's what science says:
Ginkgo Biloba
- Most studied supplement
- Multiple RCTs show no benefit over placebo
- Verdict: Don't waste your money
Zinc
- May help if zinc deficient
- Simple blood test can check levels
- Verdict: Test first, supplement if low
Magnesium
- Theoretical benefit for noise-induced tinnitus
- Limited evidence
- Verdict: Relatively safe to try
Lipoflavonoids
- Heavily marketed
- No credible evidence
- Verdict: Save your money
B Vitamins
- B12 deficiency can cause tinnitus
- Other B vitamins less clear
- Verdict: Check B12 levels
Chapter 8: The Truth About "Cures"
Let's address the elephant in the room: cure claims. Every week, patients show me advertisements for "breakthrough" cures. Here's how to evaluate them:
Red Flags for Scams
- "Ancient secret" or "Doctors hate this"
- Testimonials without scientific studies
- "Works for all types of tinnitus"
- Expensive with money-back guarantees
- Multi-level marketing structure
Why There's No Universal Cure (Yet)
Tinnitus is a symptom, not a disease. It's like asking for a cure for "pain"—the treatment depends entirely on the cause. We don't have a cure because:
- Multiple mechanisms: Different types require different approaches
- Brain involvement: Not just an ear problem
- Individual variation: What helps one person may not help another
- Chronic changes: Long-term tinnitus involves brain reorganization
The "Cures" That Aren't
Ear Candling
- Dangerous and ineffective
- Can cause burns, blockages
- Zero scientific support
Tinnitus Retraining Therapy Devices ($3000-5000)
- Some benefit for some people
- Not superior to much cheaper alternatives
- Often includes useful counseling component
Hyperbaric Oxygen
- May help acute noise trauma (first 3 months)
- No benefit for chronic tinnitus
- Expensive and time-consuming
Acupuncture
- Studies show no benefit beyond placebo
- Placebo effect can be powerful though
- Safe if you want to try
Part III: Evidence-Based Management

Chapter 9: Cognitive Behavioral Therapy: The Gold Standard
Across randomized trials and systematic reviews, one treatment consistently rises above the rest for tinnitus distress: Cognitive Behavioral Therapy (CBT). Not because it's perfect, but because it keeps holding up under scrutiny.
Why CBT Works: The Science
CBT doesn't eliminate tinnitus—it changes your brain's response to it. Think of it like learning to live in a noisy city. The traffic doesn't disappear, but your brain stops treating every car horn as a threat.
Neuroscience helps explain why CBT can work even when the sound remains:
- Threat response softens (less fear and alarm around the sound)
- Top-down control improves (better attention and emotional regulation)
- Rumination drops (less constant checking and monitoring)
The Core Components
1. Cognitive Restructuring
Catastrophic thought: "This tinnitus will ruin my life" Restructured thought: "This is challenging, but I can learn to manage it"
Catastrophic thought: "I'll never sleep again" Restructured thought: "Some nights are harder, but I've slept before and will again"
2. Behavioral Activation
Instead of avoiding activities due to tinnitus:
- Gradual re-engagement with enjoyable activities
- Building positive experiences despite tinnitus
- Breaking the isolation cycle
3. Relaxation Training
Not just "relax and it will go away," but specific techniques:
- Progressive muscle relaxation
- Diaphragmatic breathing
- Guided imagery
4. Sleep Hygiene Optimization
- Consistent sleep schedule
- Bedroom environment control
- Specific techniques for tinnitus-related insomnia
The Evidence Is Overwhelming
Let me share the findings that changed my practice:
- Large randomized evidence supports CBT-based care over usual care in real tinnitus clinics (Cima et al., 2012)
- The strongest overall review found that CBT reduces tinnitus distress and quality-of-life burden across 28 randomized trials (Fuller et al., 2020)
- Different CBT formats can work, including individual, group, and internet-delivered care (Landry et al., 2020)
- Guided digital CBT is credible, not a watered-down substitute (Beukes et al., 2022)
DIY CBT Techniques You Can Start Today
The 5-5-5 Breathing Technique
- Breathe in for 5 seconds
- Hold for 5 seconds
- Breathe out for 5 seconds
- Repeat 5 times
Why it works: Activates parasympathetic nervous system, reducing stress response
The Tinnitus Journal Track daily:
- Tinnitus loudness (1-10)
- Distress level (1-10)
- Sleep quality
- Activities that helped
- Triggers noticed
Why it works: Identifies patterns, shows progress over time
Attention Shifting Exercise
- Focus on your tinnitus for 30 seconds
- Shift attention to your breathing for 30 seconds
- Shift to sounds in your environment for 30 seconds
- Shift to physical sensations for 30 seconds
- Repeat cycle
Why it works: Trains brain that you control attention, not tinnitus
Chapter 10: Sound Therapy and Masking
Sound therapy is CBT's perfect partner—while CBT changes your brain's response, sound therapy provides immediate relief.
The Science of Sound Therapy
Your auditory system craves input. In silence, tinnitus has no competition. Sound therapy works by:
- Masking: Covering the tinnitus
- Habituation: Training the brain to ignore tinnitus
- Neuromodulation: Actually changing neural firing patterns
Types of Sound Therapy
White Noise
- Equal energy across all frequencies
- Like TV static
- Best for: High-pitched tinnitus
Pink Noise
- More energy in lower frequencies
- Like steady rainfall
- Best for: Natural, less harsh masking
Brown Noise
- Even more low-frequency emphasis
- Like ocean waves
- Best for: Low-pitched tinnitus, sleep
Nature Sounds
- Psychologically calming
- Variable and interesting
- Best for: Relaxation and stress reduction
Notched Music
- Your favorite music with tinnitus frequency removed
- Trains brain to reduce activity at that frequency
- Best for: Tonal tinnitus with identifiable pitch
Sound Therapy Best Practices
Volume Setting: The Mixing Point
- Set volume just below your tinnitus
- Should blend, not mask completely
- Complete masking prevents habituation
Duration: Consistency Beats Intensity
- Better: 2 hours daily for months
- Worse: 8 hours once a week
- Minimum: 1 hour per day
Environment Matching
- Quiet office: Soft pink noise
- Bedroom: Brown noise or nature sounds
- Exercise: Upbeat notched music
Sound Therapy Devices
Hearing Aids ($1,000-6,000)
- Amplify environmental sounds
- Many include tinnitus programs
- Essential if hearing loss present
Sound Generators ($50-500)
- Dedicated tinnitus maskers
- Worn like hearing aids
- Programmable for your tinnitus
Smartphone Apps (Free-$20/month)
- Convenient and customizable
- Quality varies widely
- Great for experimenting
Bedside Devices ($30-200)
- Sleep-focused features
- Timer functions
- Pillow speakers available
Chapter 11: Mindfulness and Meditation
I was skeptical about meditation until I saw how often it helped patients stop escalating the distress loop around tinnitus.
Why Mindfulness Works
Mindfulness doesn't make tinnitus disappear—it changes your relationship with it. Instead of fighting the sound (which paradoxically makes it louder), you acknowledge it without judgment.
Research on mindfulness-based tinnitus programs is encouraging, though the evidence base is still smaller than the CBT literature. In a randomized trial, mindfulness-based cognitive therapy reduced tinnitus severity more than relaxation training and also improved distress and disability (McKenna et al., 2017).
What people often notice after several weeks of consistent practice is:
- Improved sleep quality
- Reduced anxiety and depression
- Less automatic struggle with the sound
The Basic Practice
Mindfulness-Based Tinnitus Reduction (MBTR)
Week 1-2: Breath Awareness
- Sit comfortably, eyes closed
- Focus on breath sensation at nostrils
- When tinnitus intrudes, note "hearing" and return to breath
- Start with 5 minutes, build to 20
Week 3-4: Body Scan
- Lie down, eyes closed
- Systematically notice sensations from toes to head
- Include tinnitus as just another sensation
- Neither push away nor focus on it
Week 5-6: Sound Meditation
- Sit quietly
- Notice all sounds: tinnitus, environment, breathing
- Treat all sounds equally
- No sound is good or bad, just present
Week 7-8: Open Awareness
- Sit comfortably
- Be aware of everything: thoughts, sensations, sounds
- Tinnitus becomes one small part of total experience
- Practice "zooming out" perspective
Common Obstacles and Solutions
"I can't stop thinking"
- That's normal and fine
- Noticing thoughts IS mindfulness
- Return to breath without judgment
"Tinnitus gets louder when I meditate"
- Initially common as you stop avoiding
- Usually decreases after 2-3 weeks
- Try shorter sessions initially
"I don't have time"
- 5 minutes better than 0 minutes
- Integrate into daily activities
- Mindful walking, eating, showering
Chapter 12: Sleep Strategies That Actually Work
Poor sleep makes tinnitus worse. Worse tinnitus disrupts sleep. Breaking this cycle is crucial.
The Tinnitus-Sleep Connection
During sleep, your brain performs critical maintenance:
- Clears metabolic waste
- Consolidates memories
- Regulates neurotransmitters
Without quality sleep:
- Tinnitus perception increases
- Emotional regulation fails
- Stress hormones elevate
- Cognitive coping diminishes
The Sleep Protocol That Works
Phase 1: Environmental Optimization (Week 1)
Temperature: 65-68°F (18-20°C)
- Cool environment promotes deep sleep
- Use breathable bedding
- Consider cooling mattress pad
Darkness: Complete blackout
- Blackout curtains or eye mask
- Cover LED lights
- No screens 1 hour before bed
Sound Environment: Consistent, not silent
- Sound machine with timer (or all night)
- Set below tinnitus level
- Same sound every night for conditioning
Phase 2: Behavioral Changes (Week 2-3)
Sleep Schedule: Military precision
- Same bedtime and wake time daily (yes, weekends too)
- No naps after 3 PM
- 15-minute earlier bedtime each week if sleep deprived
The 20-Minute Rule
- Can't sleep after 20 minutes? Get up
- Do boring activity in dim light
- Return when sleepy
- Breaks anxiety association with bed
Pre-Sleep Routine: 90 minutes
- 9:00 PM: Screens off, dim lights
- 9:30 PM: Warm shower/bath
- 10:00 PM: Relaxation practice
- 10:30 PM: Bed
Phase 3: Cognitive Techniques (Week 3-4)
Worry Time
- Schedule 15 minutes daily for tinnitus concerns
- Write worries down
- Problem-solve what you can
- Acknowledge what you can't
Sleep Restriction Therapy
- Temporarily reduce time in bed
- Increase sleep pressure
- Gradually extend as sleep improves
- Counterintuitive but effective
Emergency Sleep Kit for Bad Nights
When tinnitus is screaming and sleep seems impossible:
- Get up - Don't lie there suffering
- Cool down - Splash cold water on wrists
- Gentle stretch - 5 minutes, no vigorous exercise
- Warm milk or chamomile tea - Ritual matters more than ingredients
- Read fiction - Not self-help or news
- Return when genuinely sleepy - Not just tired
Sleep Aids: Use With Caution
Melatonin (0.5-3mg)
- Start low, 2 hours before bed
- Can help reset sleep cycle
- Generally safe for short-term use
Prescription Sleep Aids
- Should be last resort
- Risk of dependence
- Can affect sleep architecture
- Discuss with doctor
Part IV: Living Well With Tinnitus
Chapter 13: Diet, Exercise, and Lifestyle Factors
Your daily choices profoundly impact tinnitus. Not through miracle cures, but through systemic effects on inflammation, blood flow, and stress.
The Anti-Inflammatory Diet
Inflammation worsens tinnitus. An anti-inflammatory diet helps:
Increase:
- Omega-3 fatty acids (salmon, walnuts, chia seeds)
- Antioxidants (berries, dark leafy greens)
- Whole grains
- Lean proteins
- Water (dehydration worsens tinnitus)
Decrease:
- Processed foods
- Excessive sugar
- Trans fats
- Excessive alcohol
- High sodium (if blood pressure sensitive)
The Caffeine Controversy
- Studies show no universal effect
- Individual variation huge
- Try 2-week elimination
- If no improvement, enjoy your coffee
Exercise: Your Secret Weapon
Exercise improves tinnitus through multiple mechanisms:
- Increases blood flow to inner ear
- Reduces stress hormones
- Improves sleep quality
- Releases endorphins
- Provides positive distraction
The Optimal Exercise Prescription:
- Aerobic: 150 minutes moderate or 75 minutes vigorous weekly
- Strength: 2 sessions weekly
- Flexibility: Daily stretching
- Mind-body: Yoga or tai chi weekly
Exercise Precautions:
- Avoid extreme loud gyms
- Use musician's earplugs if needed
- Stay hydrated
- Some report temporary spike after intense exercise (usually harmless)
Lifestyle Modifications That Matter
Stress Management
- Stress doesn't cause tinnitus but amplifies it
- Regular stress reduction mandatory, not optional
- Find what works: exercise, hobbies, therapy, meditation
Jaw and Neck Care
- TMJ dysfunction can meaningfully aggravate tinnitus for some people
- Avoid gum chewing, nail biting
- Consider night guard if grinding
- Neck stretches and good posture help
Smoking Cessation
- Nicotine constricts blood vessels
- Reduces oxygen to inner ear
- Increases inflammation
- Quitting often improves tinnitus
Chapter 14: Protecting Your Hearing
Prevention of further damage is crucial. Every decibel of hearing you preserve makes tinnitus management easier.
Understanding Dangerous Noise Levels
Safe Exposure Times:
- 85 dB (city traffic): 8 hours
- 90 dB (lawn mower): 2 hours
- 95 dB (motorcycle): 47 minutes
- 100 dB (rock concert): 15 minutes
- 110 dB (chain saw): 1.5 minutes
- 120 dB (sirens): Immediate damage possible
Smart Protection Strategies
The 2-Foot Rule If you must raise your voice to be heard by someone 2 feet away, use protection
Types of Protection:
Foam Earplugs (NRR 25-33)
- Cheap and effective
- Must insert properly (roll, pull, hold)
- Good for concerts, power tools
Musician's Earplugs ($15-200)
- Reduce volume evenly across frequencies
- Preserve sound quality
- Essential for music lovers
Electronic Earmuffs ($50-300)
- Allow conversation
- Block sudden loud sounds
- Great for shooting, workshop
Double Protection For extreme noise (>100 dB): earplugs + earmuffs
Common Noise Hazards
Often Overlooked:
- Hair dryers (85-90 dB)
- Vacuum cleaners (75-85 dB)
- Blenders (80-90 dB)
- Movie theaters (85-105 dB)
- Sporting events (90-110 dB)
- Headphones at max volume (100-110 dB)
Chapter 15: Technology and Apps
The digital revolution has democratized tinnitus management. Quality tools once requiring expensive equipment now fit in your pocket.
Tinnitus Management Apps
Clinical-Grade Apps:
Cognitive Behavioral Therapy Apps
- Structured programs based on research
- Progress tracking
- Usually subscription-based
- Some insurance coverage available
Sound Therapy Apps
- Customizable soundscapes
- Notched music therapy
- Sleep timers
- Background play capability
Combination Apps
- CBT + sound therapy
- Comprehensive approach
- Higher engagement rates
- Best overall outcomes
Evaluation Criteria for Apps
Before downloading, check:
- Evidence base (published studies?)
- Healthcare professional involvement
- Privacy policy (health data sensitive)
- Cost structure (free trial?)
- User reviews from tinnitus sufferers
- Regular updates and support
Wearable Technology
Smart Watches
- Stress monitoring
- Sleep tracking
- Breathing reminders
- Noise exposure alerts
Sleep Trackers
- Identify sleep disruptions
- Correlate with tinnitus severity
- Guide sleep optimization
Emerging Technologies
Bimodal Stimulation Devices
- Combine sound and electrical stimulation
- Early research promising
- FDA clearance beginning
Virtual Reality Therapy
- Immersive distraction
- Relaxation environments
- Early research phase
Chapter 16: Building Your Support Network
Tinnitus can be isolating. Building support systems is therapeutic, not optional.
Professional Support Team
Core Team:
- Primary Care Physician: Coordinate care, rule out causes
- Audiologist: Hearing evaluation, device fitting
- ENT/Neurotologist: Specialized evaluation
- Mental Health Professional: CBT, coping strategies
Extended Team (As Needed):
- Sleep specialist
- Neurologist
- Physical therapist (TMJ, neck issues)
- Nutritionist
Peer Support
Online Communities
- Tinnitus Talk (largest forum)
- Reddit r/tinnitus
- Facebook groups (choose carefully)
- Discord servers
Guidelines for Online Support:
- Avoid negative echo chambers
- Focus on success stories
- Be skeptical of cure claims
- Share what works, not just what doesn't
Local Support Groups
- American Tinnitus Association chapters
- Hospital-sponsored groups
- Hearing loss associations
Family and Friends
How to Help Them Help You:
Education
- Share this guide's key points
- Explain tinnitus isn't "just ignore it"
- Describe your specific challenges
Specific Requests
- "Please lower the TV volume"
- "I need to leave if it gets too loud"
- "Let's choose quieter restaurants"
What Not to Say to Someone with Tinnitus:
- "Just ignore it"
- "It's all in your head"
- "At least you're not deaf"
- "My uncle cured his with [insert remedy]"
Part V: The Future
Chapter 17: Emerging Treatments
The tinnitus treatment landscape is evolving rapidly. Here's what's on the horizon.
Near-Term (Available Now or Within 2 Years)
Bimodal Neuromodulation
- How it works: Combines sound and electrical stimulation
- Evidence: Promising early trials
- Devices: Lenire (available in Europe), others coming
- My assessment: Cautiously optimistic for subset of patients
Improved CBT Delivery
- AI-powered personalization
- Virtual reality integration
- 24/7 availability
- My assessment: Game-changer for accessibility
Pharmacological Advances
- NMDA receptor antagonists
- Potassium channel modulators
- Novel antidepressants targeting tinnitus
- My assessment: Some will help specific subtypes
Medium-Term (3-5 Years)
Gene Therapy
- Target: Regenerate inner ear hair cells
- Current status: Animal trials successful
- Challenges: Delivery to human cochlea
- My assessment: Revolutionary if successful
Brain Stimulation Techniques
- Transcranial magnetic stimulation (TMS)
- Transcranial direct current stimulation (tDCS)
- Deep brain stimulation (DBS) for severe cases
- My assessment: Promising for treatment-resistant cases
Objective Tinnitus Measurement
- Brain imaging biomarkers
- Enables precise treatment matching
- Tracks treatment response objectively
- My assessment: Will transform clinical trials
Long-Term (5-10 Years)
Hair Cell Regeneration
- Multiple approaches in development
- Would address root cause for many
- Technical challenges remain
- My assessment: The holy grail, but patience required
Precision Medicine
- Genetic testing for tinnitus subtyping
- Personalized treatment algorithms
- Predictive response modeling
- My assessment: The future of all medicine, including tinnitus
Chapter 18: Your Personal Action Plan
After 10,000 words, let's distill this into action. Here's your evidence-based roadmap.
Week 1-2: Assessment and Foundation
Medical:
- Schedule doctor appointment if criteria met (Chapter 5)
- List all medications for review
- Get hearing tested
Tracking:
- Start tinnitus diary
- Download tracking app
- Identify your triggers
Immediate Relief:
- Set up bedroom sound therapy
- Practice 5-5-5 breathing
- Implement sleep hygiene basics
Week 3-4: Building Your Toolkit
Cognitive:
- Start CBT exercises (self-help or app)
- Practice thought restructuring
- Begin attention shifting exercises
Behavioral:
- Establish exercise routine
- Optimize diet
- Build relaxation practice
Sound:
- Experiment with sound types
- Find your optimal masking level
- Create sound library
Month 2-3: Deepening Practice
Advanced Techniques:
- Add mindfulness meditation
- Try progressive muscle relaxation
- Implement sleep restriction if needed
Professional Support:
- Consider professional CBT
- Join support group
- Evaluate hearing aids if applicable
Lifestyle:
- Address TMJ/neck issues
- Reduce identified triggers
- Build positive activities
Month 3-6: Long-term Management
Optimization:
- Refine what works
- Discontinue what doesn't
- Track progress trends
Maintenance:
- Regular practice schedule
- Periodic reassessment
- Stay informed on new treatments
Your Personal Tinnitus Management Plan
Fill in your specific plan:
My tinnitus type: _________________ My main triggers: _________________ My worst time of day: _________________ My sleep disruptors: _________________
My daily practice will include:
- Morning: _________________
- Afternoon: _________________
- Evening: _________________
- Bedtime: _________________
My support team:
- Doctor: _________________
- Audiologist: _________________
- Therapist: _________________
- Support person: _________________
My success metrics:
- Week 1 goal: _________________
- Month 1 goal: _________________
- Month 3 goal: _________________
- Month 6 goal: _________________
Conclusion: The Journey Forward
If you've read this entire guide, you're serious about reclaiming your life from tinnitus. That determination is your greatest asset.
I've shared everything I know—from peer-reviewed research to clinical experience to patient wisdom. The path forward isn't always easy, but it's well-lit by evidence and walked by millions before you.
Remember:
- You're not broken - Your brain is trying to help, just misdirected
- You're not alone - millions of Americans live with tinnitus
- You're not helpless - Multiple evidence-based tools exist
- You're not defined by tinnitus - It's something you have, not who you are
The patients who thrive don't wait for a cure. They use available tools, adapt strategies to their needs, and gradually shift from fighting tinnitus to living fully despite it. Some even report becoming stronger, more resilient people through the journey.
Your tinnitus might not disappear. But your suffering can diminish, your sleep can improve, your anxiety can lift, and your life can expand beyond the boundaries tinnitus tried to impose.
Start today. Start small. But start.
The ringing might continue, but so will you—stronger, wiser, and equipped with everything you need to thrive.
Resources and References
Essential Resources
Organizations:
- American Tinnitus Association (https://www.ata.org)
- British Tinnitus Association (https://tinnitus.org.uk)
- Hearing Loss Association of America (https://www.hearingloss.org)
Research Databases:
- PubMed Central (https://pmc.ncbi.nlm.nih.gov)
- Cochrane Reviews (https://www.cochranelibrary.com)
- ClinicalTrials.gov
Key Scientific References
Fuller, T., et al. (2020). "Cognitive behavioural therapy for tinnitus." Cochrane Database of Systematic Reviews.
Cima, R.F., et al. (2012). "Specialised treatment based on cognitive behaviour therapy versus usual care for tinnitus." The Lancet.
Landry, E.C., et al. (2020). "Systematic Review and Network Meta-analysis of Cognitive and/or Behavioral Therapies (CBT) for Tinnitus." Otology & Neurotology.
Langguth, B., et al. (2019). "Therapeutic Approaches to the Treatment of Tinnitus." Annual Review of Pharmacology and Toxicology.
McKenna, L., et al. (2017). "Mindfulness-Based Cognitive Therapy as a Treatment for Chronic Tinnitus: A Randomized Controlled Trial." Psychotherapy and Psychosomatics.
Beukes, E.W., et al. (2022). "Internet-Based Audiologist-Guided Cognitive Behavioral Therapy for Tinnitus: Randomized Controlled Trial." Journal of Medical Internet Research.
Shore, S.E., et al. (2016). "Maladaptive plasticity in tinnitus: triggers, mechanisms and treatment." Nature Reviews Neurology.
Complete bibliography available at /blog/research.
About the Author
Yuan Liu, MD is a board-certified neurotologist specializing in disorders of hearing and balance. He developed Reductinn to make evidence-based tinnitus self-management tools easier to access outside specialty clinics.
Dr. Liu is a board-certified neurotologist practicing at Torrance Memorial Physician Network in Torrance, California.
When not seeing patients or developing digital health solutions, Dr. Liu enjoys hiking with his family and playing classical guitar—carefully, with proper hearing protection.
Thank you for reading The Complete Guide to Tinnitus Relief. Share this guide with anyone who might benefit.
For ongoing support and evidence-based CBT techniques, download the Reductinn app, where this guide's principles come to life through interactive exercises, progress tracking, and personalized support.
Download Reductinn:
- iOS: https://apps.apple.com/us/app/reductinn-tinnitus-relief-cbt/id6740294342
- Android: https://play.google.com/store/apps/details?id=com.mind.reductin
© 2025 Dirkes Medical, PLLC. This guide may be shared freely in its entirety with attribution.
Ready to take control?
Reductinn teaches these evidence-based techniques and more through a structured program designed by medical experts.